

Abstract
Introduction:
MM remains incurable but therapeutic advances has resulted in improved overall survival (OS) particularly for younger pts who are eligible for ASCT. Regardless OS improvements have been heterogeneous and it is well known that relapse within one year of ASCT is an independent negative prognostic factor. A particularly worse subgroup is pts who relapse and die of MM within a year of ASCT. There is limited data describing this subgroup of pts, the risk factors associated with their early relapse post ASCT and characteristics at relapse.
Objective:
Describe patient and disease related characteristics among MM pts who underwent ASCT and died of relapsed MM within the first year post ASCT in the era of novel agents.
Methods:
Pts were identified from the Leukemia/BMT Program of B.C. database, underwent ASCT between January 1st 2007 and July 31st 2016 and died of MM related causes within 365 days post ASCT. During this time period bortezomib (BORT) and lenalidomide (LEN) were available as second line therapy and BORT was available as induction pre-transplant for defined circumstances including high risk cytogenetics. Out of 752 ASCTs, 702 were performed as a part of initial therapy. The remaining ASCTs were performed as salvage or were the second of planned tandem ASCTs.
Among the remaining 702 pts 37(5.3%) died within the first 365 days post ASCT. Of the 37 pts, 32 died from MM and related causes, 2 died of TRM from ASCT and 3 died from other causes not related to MM or ASCT. The 32 pts (4.6% of the total) who died of MM and related causes were matched with 64 controls (2:1 ratio) who were selected randomly from the remaining patient cohort and matched for age, gender, and year of transplantation.
Results:
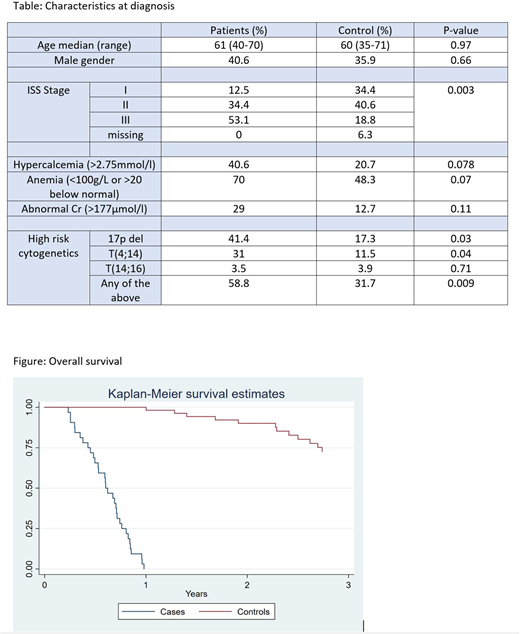
There was no difference in Age at diagnosis (Median: case 61 VS control 60, P= .97) or gender (Male case 40.6% VS control 35.9%, P= .66). There was no significant difference in the prevalence of anemia, renal dysfunction, or hypercalcemia between both groups at diagnosis (table). Pts who died within the first year of ASCT had a more advanced stage at diagnosis compared to the control group (ISS Stage III: 53.1% vs 18.8%, P= .003). BORT based induction therapy was used in 84.4% of the cases compared to 53.1% in the control group, P= .001. The majority of pts in both groups had partial response or better to frontline therapy (Cases: 81.2% VS Controls 79.7%, P= .5). Only 9.4% of cases and 4.7% of controls had evidence of disease progression at the time of ASCT. High risk cytogenetics (t(4;14), t(14;16), or del 17p) were significantly more prevalent among pts who died within the first year post ASCT compared to the control (58.82% vs 31.67%, P= .009). There was no difference in the monoclonal protein subtype between the cases and controls, P= .55. The median time from ACST to disease relapse was 118 days (40-319) for the case group compared to 511 (107-1958) in the control group.
Within the case group, 19 (59.3%) received LEN based therapy as second line therapy and 9 (28.1%) received BORT based therapy. Three patients (9.37%) were not candidates for any further therapy due to acute illness (2 sepsis, 1 subdural hemorrhage) related to fulminant MM relapse and one patient (3.1%) decided not to proceed with therapy due to functional decline. Overall, 17 pts (53.1%) received both BORT and LEN during the disease course, 12 (37.5%) received BORT only, 2 (6.25%) received LEN only and one received neither (3.1%). At the time of disease relapse, 9 (28.1%) had Hb level <85 g/l, 1 (3.1%) ANC<1000/mm3, 9 (28.1%) Plt <50/mm3, 9 (28.1%) GFR <20 ml/min, and 20 (62.5%) had at least one abnormal value (Hb, ANC, Plt, or Cr) and were not candidates for inclusion to clinical trials. Median OS (months) was Case 7.3 vs Control 63.8, P<.001.
Conclusion:
Approximately 5% of pts with MM who are ASCT eligible will die of MM within the first year post transplant. High risk cytogenetics (t(4;14), t(14;16), or del 17p) and advanced stage disease (ISS III) are risk factors for early mortality post ASCT for MM pts. These patient who relapse early typically have fulminant relapse with hematological and biochemical parameters outside of the range which would allow them to be enrolled on clinical trials and/or results in challenging standard of care management. Even in the era of novel agents, such pts do particularly poorly and represent a true unmet need in the treatment of MM. Further studies to understand the biology of their MM is required for identifying more potent therapeutic targets and protocols.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal